Many things have changed. Where do I begin?
First, I have a few more collaborators for my CRPS project now:
– Dr Andrew Burrell, VR artist
– Prof William Martens, acoustic architecture scientist, University of Sydney
– Meisha Stevens, Post Grad acoustic architecture science student, University of Sydney
– Tom Hazell, electrical engineer student, University of NSW
– Rob Yuan, design computing student, University of Sydney
In the last post, I mentioned some of the difficulties we were having designing the glove device. We still have some issues but we now have two extra engineering students to help us experiment.
The effects/sensation of CRPS we want to simulate via the glove are:
– heat
– throbbing (possibly in sync with the participant’s heart rate)
– heavy
– clammy, sweaty
– pressure
– swelling

We have found a pair of TENS gloves, which will go on the first layer – directly onto the participant’s hand.
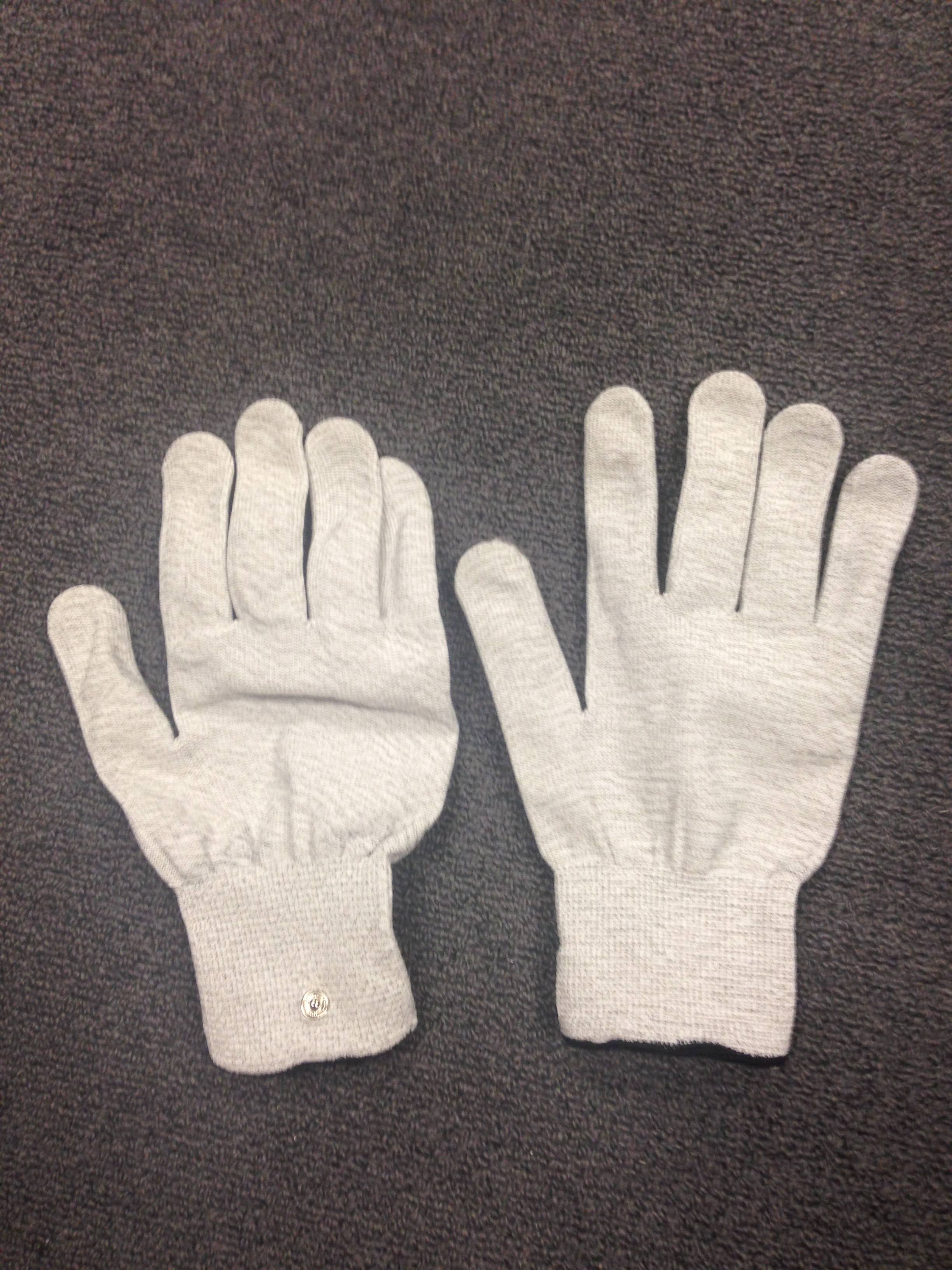
This will produce a tingling sensation that we can increase or decrease, depending on the individual’s response. Rosie Menzies (University of Sydney) and the engineering students are working on the rest of the effects. It’s tricky without bulking up the thickness of the glove, and its design has to be robust enough that the glove should be able to manage constant handling.
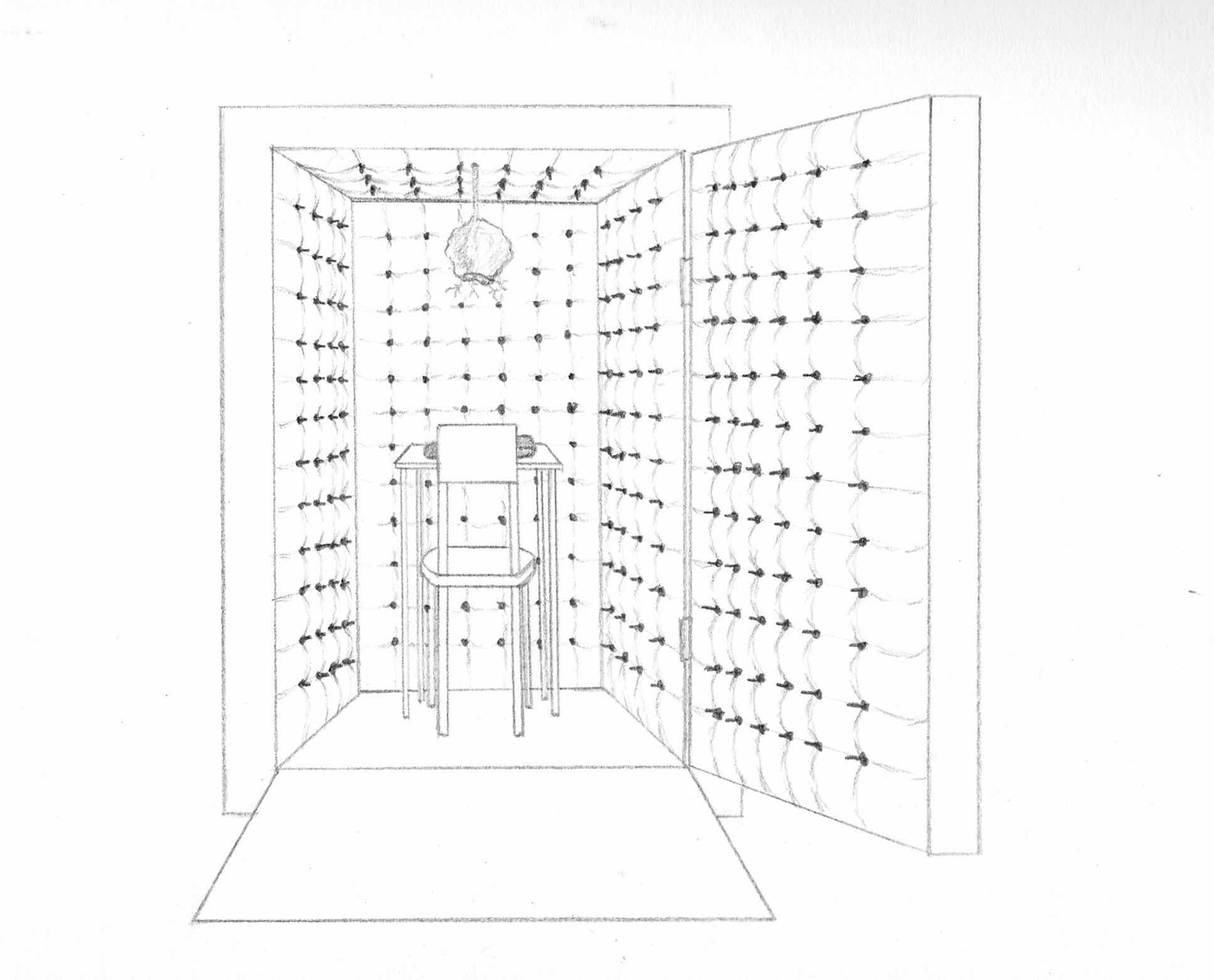
Anyhow, we’ve been doing lots of research and talking/meeting for the last few months. My idea of using rows of rotating barbed wire in a room (to enhance the anxiety) has been scrapped. What will replace it is more effective and is full of potential for my next few projects. I am now planning to build an anechoic chamber (an example here) coupled with auditory manipulation using low frequency sound to temporarily disturb the participant’s sensory and cognitive perceptions. I will probably need a couple of subwoofer speakers for this, which we will hide behind the acoustic foam. My anechoic chamber, however, is not going to look like a typical chamber with foam wedges. Instead, I’m covering the foam with a white fabric. The fabric will be tufted and pierced with short barbed wire spikes and will cover the walls and ceilings, thereby creating both the feeling of a domestic environment, since most pain patients suffer alone at home, with one where it is impossible to find a comfortable position to rest in.
So this is what happens when I take each participant into the anechoic chamber:
The influence of the acoustics in this room, with low frequency sound manipulation, symbolically simulates the altered sensory-cognitive responses of people living with chronic pain. The participant then wears a purpose-built glove and a pair of Virtual Reality (VR) goggles. With a remote control I produce selected CRPS symptoms and visual effects, felt and seen through the glove and VR. Instead of looking at the gloved hand, they will see the VR 3D hand that looks something like this:

As they feel the effects from the glove, what they see of their virtual hand will become purply red and blotchy, then progressively swollen and shiny.
Up till then, they don’t actually feel pain on their hand because those are only mechanical sensations of tight pressure, throb, very warm heat etc. They might feel uncomfortable but it will not be pain. Now, here is the thing. What they will experience next will, as my collaborating pain scientists hypothesise, feel pain because their brains will start firing pain signal to their effected limbs. This is what I’m going to do:
At the height of the effect, the participants will see, through the VR goggles, a strand of barbed wire from above slowly creeps toward the affected hand. It will continue to advance until it “touches” the virtual wrist to scrape and tear. What they won’t realise is that the actual mechanical touch onto their real hand will only be a feather-like tickle. But the visual feedback (the external threat) that their hands are being scraped and torn is so much stronger and threatening than the actual feather touch. So their brains will decide that what they are seeing is more real and in urgent need of protection, that their brain will activate pain signals to the affected hands.
In summary, this is what our research is really about. We are NOT giving pain to participants’ hands in any way. What we are studying is to find out whether we can provide just the right environment for each participant so that it is their own brains will send pain signals to their hands. I’m particularly interested in the outcome personally. Why? Because people in general think that pain is a sign of weakness. This is one of the reasons why there is so much misunderstanding and stigma attached to chronic pain. I want to show people that pain is more than a mere weak mindset. It has so much to do with the brain, and its plasticity. We think we can make most of the participants produce pain from their brains, regardless of their ‘weak’ or ‘strong’ minds. But then again, we don’t really know that yet until we actually try.
Anyhow, so what are the elements that can create that ‘just the right environment’ for pain? I had to think about this a lot. The ‘right environment’ is not only involving biological/mechanical input – like heat, pressure, touch etc. It also has to involve psychological and social factors like anxiety, stress, isolation, other people’s attitudes and relationships with others etc. The anxiety level for people with chronic pain for instance, seems always high compared to people with no pain. What I really want to include in this project is incorporating these subjective states – their anxiety, fear, anticipation, and catastrophising – and how they contribute towards creating pain narratives for each individual. I think my collaborators and I are close to bringing all these in, especially inside the anechoic chamber, but it’s all just theory at this stage.
Within the last few months, our research development has finally started to have a very tangible form, at least in our minds, and I want to involve participants in something that is both an art project and a scientific research. So this is how it will pan out:
It’s going to be an interactive performance installation that will take each participant on a one-on-one journey through three interactive rooms. Using new technologies, I invite them to experience an illusion of Complex Regional Pain Syndrome (CRPS), by temporarily manipulating their sensory and cognitive perceptions.
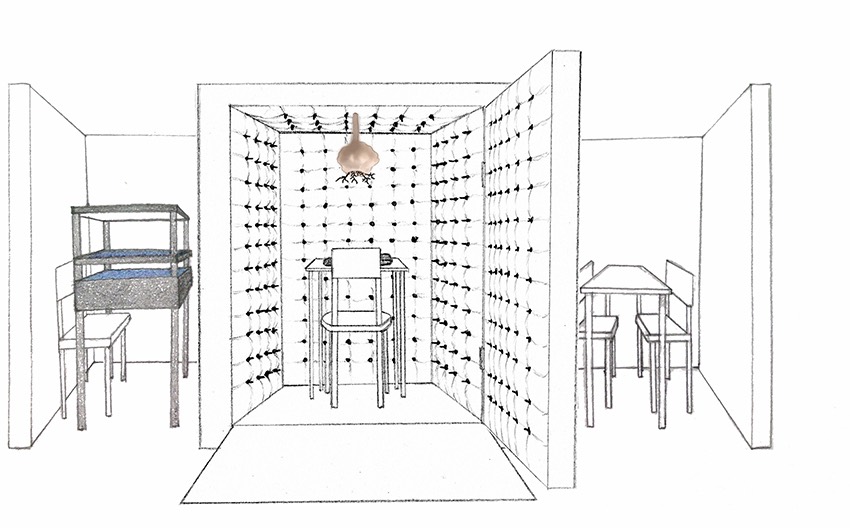
Stage1-Room1: a simple Augmented Reality play using a Mirage Machine (read the previous post, Establishment and Development) makes their hands ‘disappear’ – a method used for neuroscience study – psychologically priming them for Stage 2.
Stage2-Room2: an anechoic chamber that deceptively looks more like a domestic setting. The influence of the acoustics in this room, with low frequency sound manipulation, symbolically simulates the altered sensory-cognitive responses of people living with chronic pain. The participant wears a purpose-built glove and a pair of Virtual Reality (VR) goggles. With a remote control I produce selected CRPS symptoms and visual effects, felt and seen through the glove and VR.
Stage3-Room3: evaluate the participant’s responses with questionnaires and share the concept behind the artwork.
There are a lot of collaborators working on this project, and it’s nearly time to put everything together. It’s been relatively smooth sailing so far, so I hope it continues that way.